Health workers say the reuse of syringes drove the outbreak in the city of Ratodero.

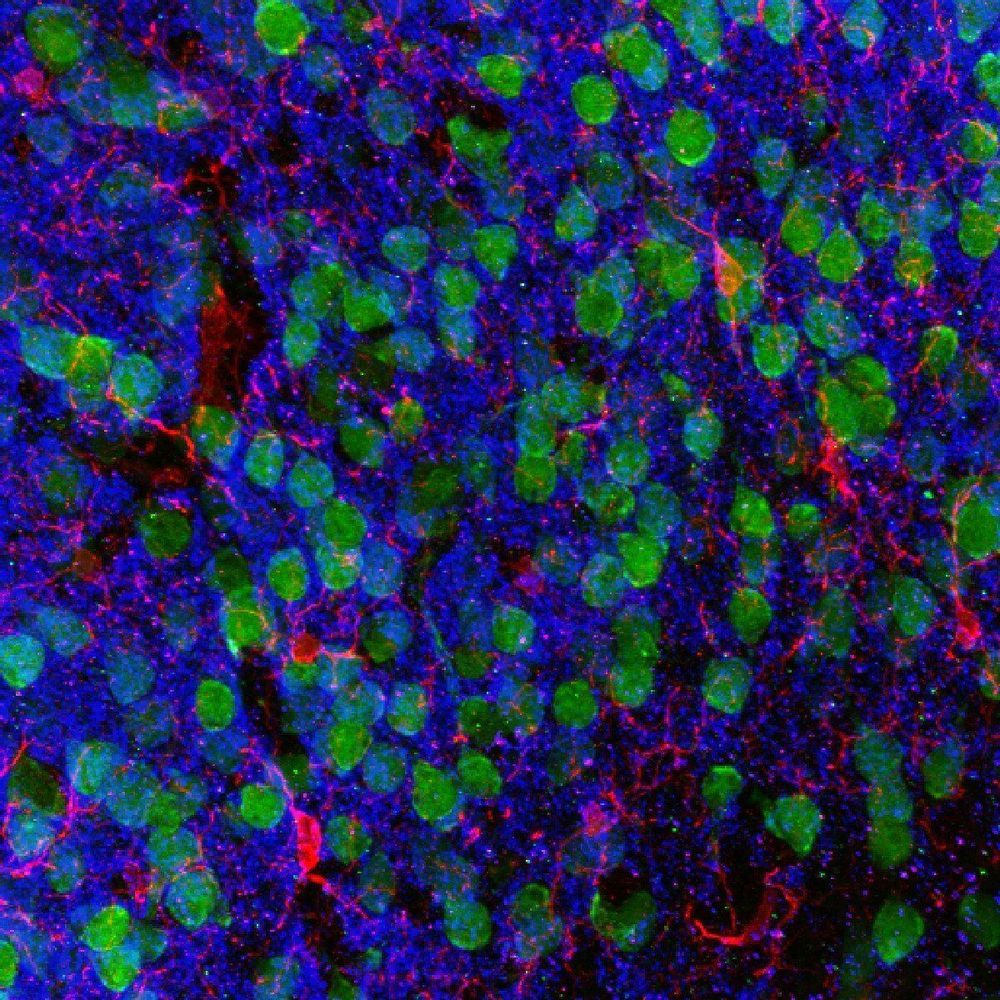
New cellular and molecular processes underlying communication between gut microbes and brain cells have been described for the first time by scientists at Weill Cornell Medicine and Cornell’s Ithaca campus.
Over the last two decades, scientists have observed a clear link between autoimmune disorders and a variety of psychiatric conditions. For example, people with autoimmune disorders such as inflammatory bowel disease (IBD), psoriasis and multiple sclerosis may also have depleted gut microbiota and experience anxiety, depression and mood disorders. Genetic risks for autoimmune disorders and psychiatric disorders also appear to be closely related. But precisely how gut health affects brain health has been unknown.
“Our study provides new insight into the mechanisms of how the gut and brain communicate at the molecular level,” said co-senior author Dr. David Artis, director of the Jill Roberts Institute for Research in Inflammatory Bowel Disease, director of the Friedman Center for Nutrition and Inflammation and the Michael Kors Professor of Immunology at Weill Cornell Medicine. “No one yet has understood how IBD and other chronic gastrointestinal conditions influence behavior and mental health. Our study is the beginning of a new way to understand the whole picture.”

Two major U.S. biomedical research funders plan to each put at least $100 million over 4 years toward bringing cutting-edge, gene-based treatments to a part of the world that often struggles to provide access to even basic medicines: sub-Saharan Africa. The National Institutes of Health (NIH) and the Bill & Melinda Gates Foundation today announced the unusual collaboration to launch clinical trials for gene-based cures for HIV and sickle cell disease within the region in the coming decade.
The ambitious goal is to steer clear of expensive, logistically impractical strategies that require stem cell transplantation, and instead develop simpler, affordable ways of delivering genes or gene-editing drugs that can cure these diseases. “Yes, this is audacious,” NIH Director Francis Collins said during a press teleconference this morning on the project. “But if we don’t put our best minds, resources, and visions together right now, we would not live up to our mandate to bring the best science to those who are suffering.”
After decades of work and setbacks, the traditional gene therapy approach of delivering DNA into the body to replace a defective gene or boost a protein’s production is now reaching the clinic for several diseases, including inherited blindness, neuromuscular disease, and leukemia. Animal studies and some clinical trials have suggested that two diseases prevalent in Africa, HIV and sickle cell disease, can be treated by gene therapies or newer genome-editing tools such as CRISPR.


Marketing always starts with Demand (Reuters) — http://Amazon.com/ Inc said on Wednesday it bought healthcare start-up Health Navigator, its second purchase in the healthcare services industry.
(Reuters) — Amazon.com Inc said on Wednesday it bought healthcare start-up Health Navigator, its second purchase in the healthcare services industry.
The deal comes after the company acquired online pharmacy PillPack last year, pitting itself against drugstore chains, drug distributors and pharmacy benefit managers. (reut.rs/31DSU8k)
The company said the acquisition is a part of its new employee offering, Amazon Care, where employees of the e-commerce giant will be able to receive fast-paced access to healthcare facilities without having to make appointments.

Just in time for Halloween, doctors in France say they witnessed a real-life horror tale involving an antibiotic-resistant superbug. In less than a month, their patient’s infection evolved resistance to the last-resort drug they had used to treat it. Thankfully, the doctors were still able to defeat the microscopic threat—and the case may have uncovered a peculiar weakness in the germ.
According to the report, published in the journal Antimicrobial Agents and Chemotherapy, a young child had been dealing with recurrent infections of the bacteria Pseudomonas aeruginosa for over two years. P. aeruginosa is an opportunistic infection that sickens tens of thousands of already weakened people in hospitals and other health-care settings in the U.S. a year. In these people, it can cause serious infections.

United Parcel Service Inc. is striking a series of drone-delivery agreements with health-care groups as it develops new technology pitched to the growing medical market.
The plans include expanding the use of drones to deliver cargo such as medical samples and supplies on hospital campuses in Utah and elsewhere, and an agreement with CVS Health Corp. to evaluate the use of drones for home delivery of prescriptions and other products, UPS said Monday.
The agreements are the first UPS has announced since the package delivery giant won U.S. regulatory approval to operate commercial drone flights through the company’s Flight Forward subsidiary. The nod from the Federal Aviation Administration paves the way for UPS to scale up operations as it competes with FedEx Corp., Amazon.com Inc. and others vying to develop drone delivery services in the U.S.

Listen to The A Level Biologist Podcasts episodes free, on demand. As we enter the golden age of life science we should not just keep getting sick and dying. Too much to ask for?Learn more about Aubrey and SRF at https://www.sens.orgFull transcript: https://thealevelbiologist.co.uk/indefinite-health-with-dr-aubrey-de-grey/The A Level Biologist Podcasts is brought to you by The A Level Biologist — Your Hub @ https://thealevelbiologist.co.ukSupport the show. The easiest way to listen to podcasts on your iPhone, iPad, Android, PC, smart speaker – and even in your car. For free. Bonus and ad-free content available with Stitcher Premium.