For the first time, carbon dioxide and carbon monoxide ices have been observed in the far reaches of our solar system on trans-Neptunian objects (TNOs).


Users simply register by taking a selfie and then verify their identity and payment transaction by looking at the restaurant’s camera, according to CNBC.
In essence, it acts very similar to Apple’s Face ID.
The Cali-based software company explained the tech on its website, reading: ‘PopID is the universal gateway for verifying an individual’s identity based on their face for applications such as loyalty and payment.’
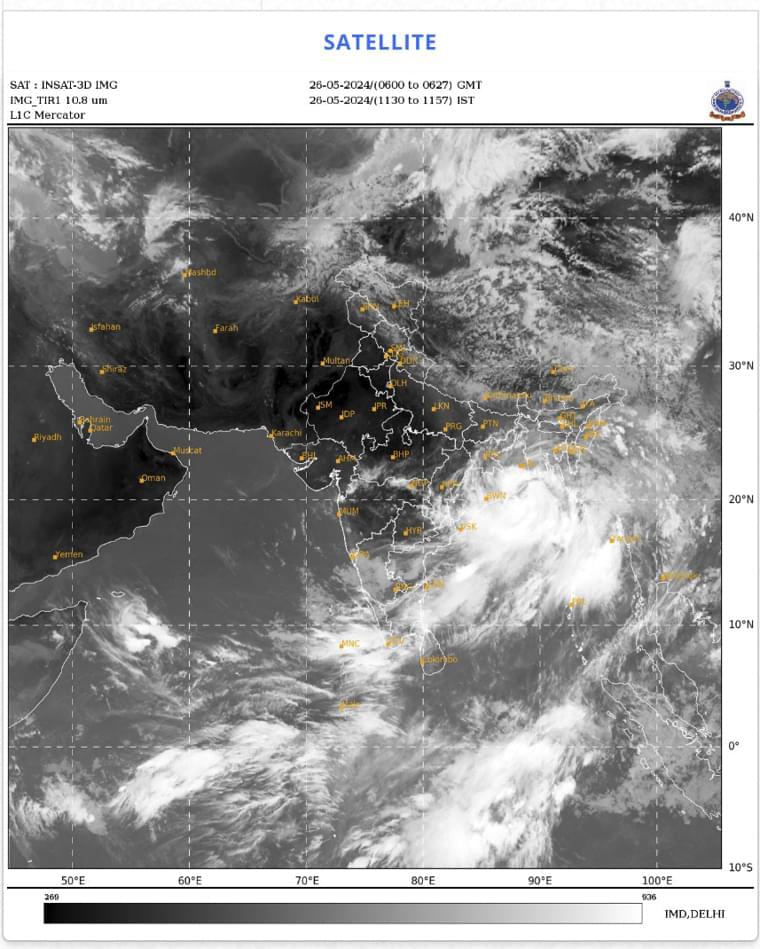
NEW DELHI (AP) — Bangladesh evacuated nearly 800,000 people from vulnerable areas on Sunday as the country and neighboring India awaited the arrival of a severe cyclone that has formed over the Bay of Bengal. The storm is expected to cross Bangladesh and India’s West Bengal coasts around midnight Sunday. The India Meteorological Department said it is expected to reach maximum wind speeds of up to 120 kilometers per hour (75 mph), with gusts up…
This fun and innovative project employs a rotary encoder and Arduino to capture rotational data and translate it into car movements in VR.
“If you frame it as an either/or question, it’s too simplistic,” says Utah State University evolutionary biologist Zachariah Gompert. “The answer isn’t ‘completely random’ or ‘completely deterministic and predictable.’ And yet, examining short time scales, we can find predictable, repeatable evolutionary patterns.”
Gompert and colleagues report evidence of repeatable evolution in populations of stick insects in the May 24, 2024, online edition of the American Association for the Advancement of Science’s journal Science Advances. Collaborating authors on the paper include Gompert’s long-time collaborator Patrik Nosil and other researchers from France’s University of Montpelier, Brazil’s Federal University of São Paulo, the University of Nevada, Reno and Notre Dame University. The research is supported by the National Science Foundation and the European Research Council.
The team examined three decades of data on the frequency of cryptic color-pattern morphs in the stick insect species Timema cristinae in ten naturally replicate populations in California. T. cristinae is polymorphic in regard to its body color and pattern. Some insects are green, which allows the wingless, plant-feeding insect to blend in with California lilac (Ceanothus spinosus) shrubs. In contrast, green striped morphs disappear against chamise (Adenostoma fasciculatum) shrubs.
“Batteries are the crux of many of the most important emerging technologies in both the civilian world and, important to our profession, on the battlefield,” said United States Military Academy Cadet Michael Williams. “More energy dense batteries allow, for instance, greater range on electric vehicles, longer battery lives for radios, and longer flight times for drones. Our work helps make manufacturing these batteries easier.”
Cadets Michael Williams, Avery Patel, and Nancy Astable have been working on a long-term project with their faculty mentors Dr. Enoch Nagelli, Dr. Simuck Yuk, and Army Col. John Burpo to develop new ways to maximize energy storage and generation for the U.S. Army Combat Capabilities Development Command’s Armaments Center. In collaboration with Cornell University, the team at USMA’s Department of Chemistry and Life Sciences is pursuing innovative approaches to increasing the quality and use of batteries and fuel cells.
The value of conducting scientific research to solve real-world problems is clear to the cadets.
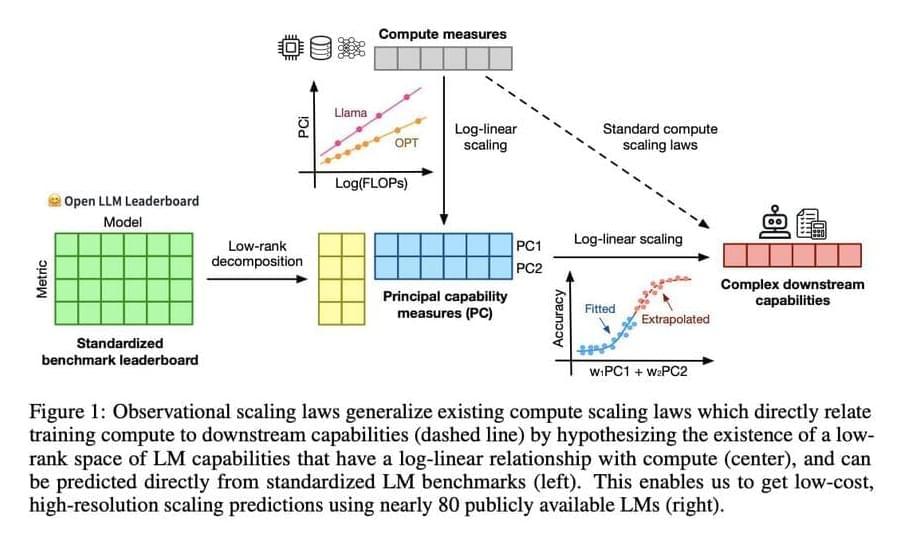
Language models (LMs) are a cornerstone of artificial intelligence research, focusing on the ability to understand and generate human language. Researchers aim to enhance these models to perform various complex tasks, including natural language processing, translation, and creative writing. This field examines how LMs learn, adapt, and scale their capabilities with increasing computational resources. Understanding these scaling behaviors is essential for predicting future capabilities and optimizing the resources required for training and deploying these models.
The primary challenge in language model research is understanding how model performance scales with the amount of computational power and data used during training. This scaling is crucial for predicting future capabilities and optimizing resource use. Traditional methods require extensive training across multiple scales, which is computationally expensive and time-consuming. This creates a significant barrier for many researchers and engineers who need to understand these relationships to improve model development and application.
Existing research includes various frameworks and models for understanding language model performance. Notable among these are compute scaling laws, which analyze the relationship between computational resources and model capabilities. Tools like the Open LLM Leaderboard, LM Eval Harness, and benchmarks like MMLU, ARC-C, and HellaSwag are commonly used. Moreover, models such as LLaMA, GPT-Neo, and BLOOM provide diverse examples of how scaling laws can be practiced. These frameworks and benchmarks help researchers evaluate and optimize language model performance across different computational scales and tasks.
Neuromorphic computing represents an exciting crossover between technology and biology, a frontier where computer science meets the mysteries of the human brain. Designed to mimic the way humans process information, this technology holds the promise to stir a revolution everywhere, from artificial intelligence to robotics. But what exactly is neuromorphic computing and why is it taking the center stage?
Those who know Oxford University for its literary luminaries might be surprised to learn that some of the most important reflections on emerging technologies come from its hallowed halls. While the leading tech innovators in Silicon Valley capture imaginations with their bold visions of future singularities, mind-machine melding, and digital immortality by 2045, they rarely engage as deeply with the philosophical issues surrounding such developments as their like-minded scholars over the pond. This essay will briefly highlight some of the key contributions of Oxford University’s professors Nick Bostrom, Anders Sandberg, and Julian Savulescu to the transhumanist movement. It will also show how this movement’s focus on radical autonomy in biotechnical enhancements shapes the wider global bioethical conversation.
As the lead author of the Transhumanist FAQ, Bostrom provides the closest the movement has to an institutional catechism. He is, in a sense, the Ratzinger of Transhumanism. The first paragraph of the seminal text emphasizes the evolutionary vision of his school. Transhumanism’s incessant pursuit of radical technological transformation is “based on the premise that the human species in its current form does not represent the end of our development but rather a comparatively early phase.” Current humans are but one intriguing yet greatly improvable iteration of human existence. Think of the first iPhone and how unattractive 2007’s most cutting-edge technology is in 2024.
In particular, transhumanists encourage radical physical, cognitive, mood, moral, and lifespan enhancements. The movement seeks to defeat humanity’s perennial enemies of aging, sickness, suffering, and death. Bostrom recognizes that he is facing the same foes as Christianity and other traditional religions. Yet he is confident that Transhumanism, through science and technology, will be far more successful than outdated superstitions. Biotechnological advances are more reliable for this worldly benefit than religion’s promises of some mysterious next life. Transhumanists claim no need for “supernatural powers or divine intervention” in their avowedly “naturalistic outlook” since they rely instead on “rational thinking and empiricism” and “continued scientific, technological, economic, and human development.” Nonetheless, Bostrom and his companions recognize that not all technology is created equal.
{kind=link}